
Inflection Points In The Parkinson's Disease Journey : A Practical Guide for Patients and Caregivers
- Lifespark
- May 16
- 4 min read

Part of the STEP 2026 World Parkinson's Day Event expert series
Delivered by Dr Anil Venkitachalam, Neurologist, Mumbai
There is a moment, often quiet and easy to miss, when Parkinson’s disease changes course. It doesn’t always announce itself dramatically. Sometimes it shows up as a near fall you brush off, a softer voice that others point out, or a new frustration with sleep that no one quite connects to Parkinson’s.
In this insightful session, Dr Anil Venkitachalam reframed the way patients and caregivers should think about the condition—not as a slow, steady decline, but as a journey marked by turning points.
“An inflection point is a time of significant change… from that point onwards, the patient has a higher chance of deterioration.”
If you can recognise these inflection points early, you can act early—and preserve quality of life.
First step, a shift in mindset. It’s not just “Parkinson’s”
One of the earliest—and most important—inflection points is understanding what diagnosis really means.
“Parkinsonism is an umbrella term… Parkinson’s disease is the most common cause, but not the only one.”
Dr Venkitachalam explained that what looks like Parkinson’s may actually be:
Atypical conditions like MSA or PSP
Secondary causes like medications or strokes
Why does this matter? Because different conditions:
Progress at different speeds
Respond differently to treatment
May or may not qualify for advanced therapies [STEP 2026...transcript | Txt]
For caregivers, this means: if something about the disease course feels “different” or unusually rapid, it is worth revisiting the diagnosis.
The iceberg problem: What you see isn’t what matters most
Most families first notice tremor. It’s visible, distressing, and often the focus of concern.
Parkinson’s is often described as an iceberg:
Above the surface: tremor, stiffness, slow movement
Below the surface: sleep problems, constipation, mood issues, dizziness, hallucinations, cognitive changes
These “invisible” symptoms are frequently what drive suffering—for both patients and caregivers.
“What we see is mainly the tip of the iceberg… what is hidden are the significant symptoms.”
Takeaway: If you focus only on what is visible, you will miss what actually affects day-to-day life.
Why tracking matters: Parkinson’s changes in “steps”
Another key idea from the session was that Parkinson’s doesn’t worsen smoothly. It changes in steps.
“Many families feel PD worsens suddenly… often an invisible symptom has crossed a threshold.”
So instead of asking, “Is the disease progressing?”, the better question is: Has something changed recently that signals a turning point?
The 4 Inflection Points That Matter Most
Dr Venkitachalam highlighted four high-impact inflection points—each one actionable if recognised early.
1. Falls & Freezing: The Safety Pivot
This is often the first major turning point.
“Near falls are a warning sign… the patient needs to report every fall.” [STEP 2026...transcript | Txt]
Falls are not just accidents. They are signals.
He described two major risks in Parkinson’s:
Falling → injury → immobility
“If you are able to treat these two important points, you will give them a good quality of life.”
What to watch for:
Near-falls or stumbles
Freezing (especially in doorways, bathrooms, turning)
Anxiety or rushing making movement worse
Dizziness, especially when standing
What you can do:
Start physiotherapy early—don’t wait
Slow down routines (especially transitions)
Get blood pressure checked lying and standing
Report every fall honestly
2. Swallowing, Speech & Breathing: The Quiet Risks
This inflection point is often overlooked until it becomes serious.
“For swallowing it should be 10 on 10… even if you choke once, you can aspirate.”
Warning signs:
Coughing with food or water
A “wet” or gurgling voice
Unexplained weight loss
Repeated chest infections
Speech changes may seem minor—but they impact communication, confidence, and social connection.
“Speech is not just ageing… therapy can help.”
Breathing symptoms may also appear—linked to medication cycles, anxiety, or swallowing issues.
What you can do:
Ask early for swallow and speech evaluation
Modify food consistency if advised
Explore structured speech therapy (e.g., LSVT)
Observe patterns in breathing discomfort
3. Non-Motor Symptoms: The Invisible Load
This is perhaps the most under-recognised inflection point.
“Non-motor symptoms are… invisible but equally important.”
These include:
Sleep disturbances
Depression, anxiety, apathy
Constipation
Urinary urgency
Hallucinations, confusion, cognitive change
A striking analogy he used:
“Sleep is like the garbage truck of your brain… it cleans your brain at night.”
What you can do:
Track a few key symptoms weekly (don’t try to track everything)
Actively report non-motor changes at doctor visits
Recognise these as part of Parkinson’s—not “just ageing”
4. Medication Changes: The Subtle Signals
Over time, medications may stop working as smoothly.
“If you are OFF often… you are under-medicated or something is wrong. If there is too much dyskinesia… the patient may be overmedicated.”
What to track:
How many hours per day symptoms are uncontrolled (OFF time)
When symptoms worsen relative to dose timing
Presence of involuntary movements (dyskinesia)
What you can do:
Keep a simple medication-response log
Discuss patterns, not just symptoms
Ask early about advanced therapies if quality of life drops
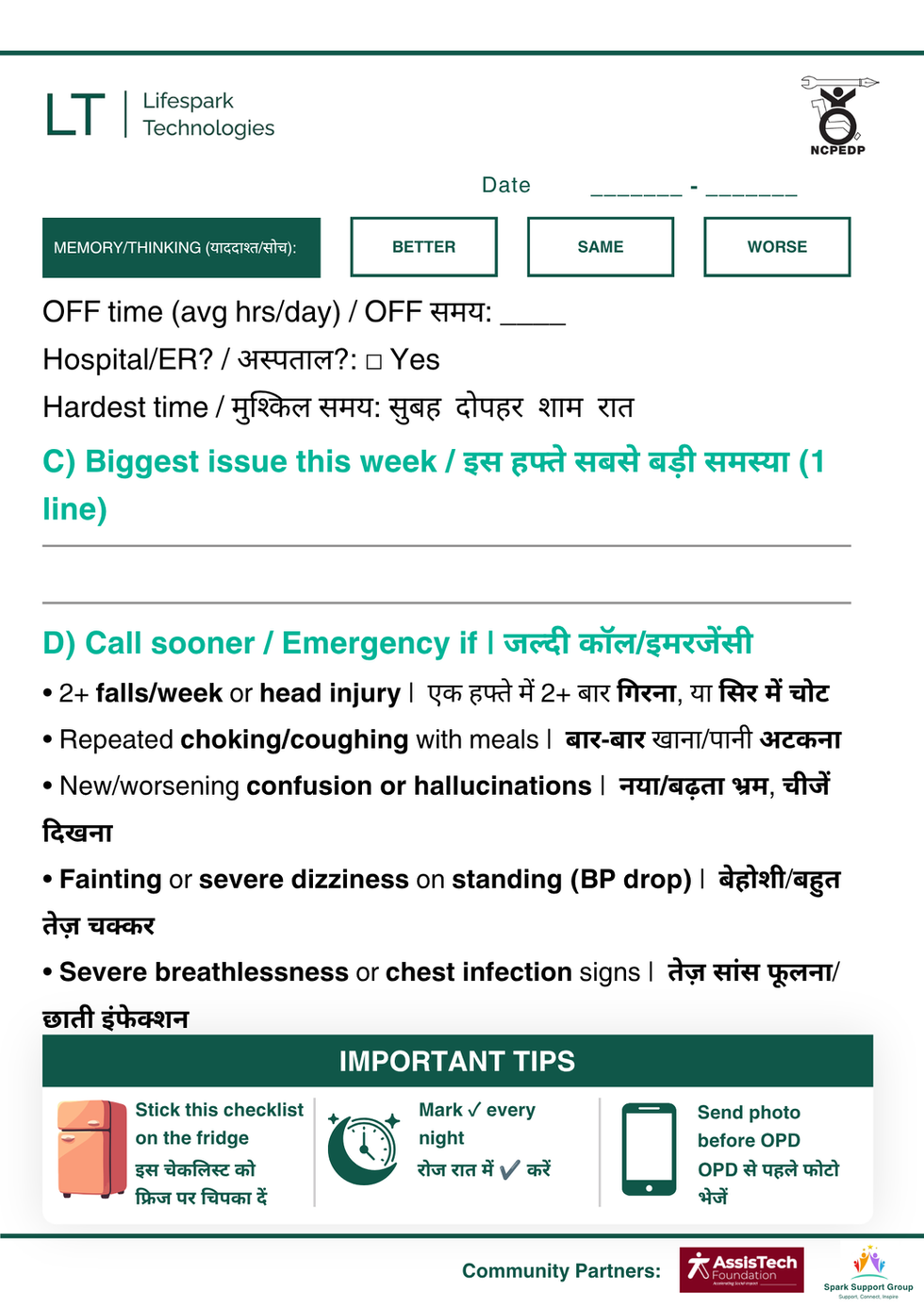
The most practical tool: A 60-second tracker
One of the most actionable ideas from the session was the simplified OPD tracker.
Instead of documenting everything, just track four areas:
Safety: falls, near-falls, dizziness
Eating & speaking: choking, soft voice, breathlessness
Non-motor: sleep, mood, constipation, confusion
Medication: OFF time, dyskinesia
“If you track these… you will know when to take preventive action.” Don’t wait if you see repeated falls, frequent choking, or new confusion.
Download the tracker below, print it and take it to your doctor visits



A final reassurance—and responsibility
Dr Venkitachalam closed with a grounded but hopeful note.
“Parkinson’s is a long disease… you can have a good quality of life.”
But that outcome depends on one thing: how actively the disease is tracked and managed.
“Focus on the hidden risks… identify them, evaluate them, and treat them.”
Because in Parkinson’s, what you notice—and when you act—can change the trajectory.
Next expert session : Proactively Managing and Improving Mobilty in Parkinson's Disease by Dr Darshan Doshi
